
Human-centric, biodynamic, chronobiologic, biophilic, circadian, melanopic… whichever term you use, they herald a new era for lighting designers, based on the non-image-forming functions of the human eye. Understanding of these functions largely dates back to the 1990s and the discovery of intrinsically photosensitive retinal ganglion cells (ipRGCs) in the retina. If these cells do not receive light for two hours, melatonin is produced, which triggers the sleep or circadian cycle. (See panel, ‘The eyes have it’).
Essentially, it means your eyes and brain receive signals from the external day/night cycle, which tell your body when to be awake and when to sleep. Many of us now spend 90% of our time indoors, in artificial light, often staring at screens for more than seven hours. So the feeling is that our connection with the outside has been lost and, with it, the spectrum of daylight that maintains a normal sleep cycle.
It’s a seductive argument; we spend more time in artificial lighting environments, and more time exposing ourselves to blue-spectrum light, when we should be relaxing in the warm glow of a candle. It is understandable that this may be impacting on our sleep patterns, and evidence does suggest that messing with the sleep cycle is bad for you, as reflected in higher rates of cancer, diabetes, ulcers and heart disease among shift or night workers.
How do we design lighting to support a circadian system? With LED light sources came the ability to dim and colour mix; these developments have run parallel with research into circadian rhythms – and so circadian lighting was born. This is a set-up – usually for offices, but sometimes for education or care environments – which carries out colour temperature and illumination change throughout the day. A sort of artificial sunrise to sunset, which travels from 2,700K to 6,500K and back again.
The eyes have it
Intrinsically photosensitive retinal ganglion cells (ipRGCs) in the retina receive light and use it to send messages about the external light/dark cycle to the rest of the body. If ipRGCs do not receive light for two hours, they send a message to the hypothalamus, which contains the suprachiasmatic nucleus (SCN), and this – via the pineal gland – starts the secretion of melatonin, so triggering the sleep, or circadian, cycle. The SCN acts as the master circadian clock, overseeing a near-perfect 12-hour-cycle timeclock in each of the body’s 37.2 trillion cells.
The photo pigment in ipRGCs is called melanopsin, and this – together with rods, and blue, red and green cones – make up our non-image-forming system within the retina. Each element is more sensitive to different wavelengths of light and values of irradiance or amount of light.
In circadian lighting terms, the ‘superstar’ wavelength is in the blue spectrum – about 480nm, the peak sensitivity of ipRGCs. The impact of blue-spectrum lighting is not new; in the late-1990s, research by lighting manufacturers suggested that a punch of blue-spectrum light would stimulate workers, rather like battery hens. It is also the dominant spectrum in daylight – and perhaps this is the key to understanding the subject.
The idea is that by providing appropriate-intensity, blue-spectrum light during the main daylight hours – and warmer spectrum when the body should be relaxing – you create an environment for melatonin suppression for alertness and cortisol release, which controls body temperature. So does it work?
A number of case studies in schools, hospitals and offices suggest that it does. Students, for example, have been said to concentrate better after the installation of a circadian-supportive lighting system, because of the colour-change element. However, in many cases, the schools previously had poor lighting and dark, dirty interiors, so the improvement could be a result of the fresh, new, well-lit interiors – after all, we know that good lighting can engage and invigorate, and doesn’t have to mix colours to do that.
Many studies rely on subjective answers from people asked directly about their response to new lighting once the system and ‘benefits’ have been explained. As a result, this evidence could be unreliable.
As a designer, I am concerned that these lighting systems are being installed now, when research is in its infancy
So although research is available, it is not entirely convincing. One of the reasons is that we don’t know what we are supposed to be testing. How do we quantify the effects and ‘doses’ of circadian lighting?
Scientists from the University of Manchester have proposed the melanopic illuminance curve of eye sensitivity. Like the Vλ curve of photopic eye sensitivity, the melanopic curve looks at wavelengths of light for melanopsin in the ipRGCs1.
This curve represents the best model for understanding the appropriate spectral wavelength for melanopsin and can be used to build the light spectrum appropriate for an internal luminaire. It is the closest we have to quantifying the spectrum required for melatonin suppression, but as the scientists state: ‘It is not always clear whether lighting design should aim to maximise or minimise non-visual responses. In many ways, light can be considered a drug, having the potential for both beneficial and deleterious effects. These conflicting effects can occur concurrently, and in a single individual and context.’ And again: ‘It is not yet possible to predict the non-image-forming impact of a given illuminant based on its intensity and spectral composition. However, some guidance is possible.’2 Even the international commission on illumination, the CIE, recently released a statement regarding clarity on the latest thinking (See panel, ‘Missing links’).
Missing links
‘Non-visual responses are subject to complex signal processing in the central nervous system and influenced by as-yet-unresolved interactions of photoreceptive units. The missing understanding of the input-output characteristics between light stimulus and the resulting non-visual response seems to make tailored light application for a desired lighting effect impossible.’
CIE statement on non-visual effects of light – Recommending Proper Light at the Proper Time.
Others are more supportive of the system. Mark Rea and his team from the Lighting Research Center, in New York, believe in the validity of circadian lighting. The Well Building Standard offers melanopic illuminance values measured vertically at face height as a key to creating healthy lighting, and the German standard – DIN Spec 6760 – offers metrics for ‘biologically effective’ lighting.
Are there risks? One issue is the one-size-fits-all approach. People are different – from our chronotype (how we sleep), to our geography, work pattern, diet, age and subjective responses to light. We know, for instance, that the eye yellows and receives less blue-spectrum light as we age, and that a person of 50-60 years secretes about 35% of the melatonin of a 10-year old.

And what about preference? Research suggests blue-spectrum light is needed, but does anyone want to work in 6,000K-8,000K artificial light? Our geography will also influence preferences; for example, the definition of cool white light in the Middle East is different from that in western European – so, if science tells us it has to be 8,000K, will we accept this? Will we bury our preference for the sake of sleep? What if we require 5,000 lux? Will our energy targets cope with additional loads?
We also have to consider whether additional blue light is OK for our eyes. Short-wavelength blue light hits the retina faster than long-wavelength light, and could cause oxidative stress in the retinal tissue. Public Health England has stated that normal LEDs are not an issue in this sense, but what if we raise blue spectrum levels? Age-related macular degeneration, the leading cause of vision loss in the UK, affects 600,000 people – and is on the rise. Could an increase in blue light spectrum be causing this?
There is also flicker. With mixing between colour sources comes dimming, and dimming often causes flicker. Many electronic drivers for LEDs have high flicker modulation, similar to that of old fluorescent lighting that a generation said gave them headaches. Could a dimming or colour-mixing system cause detrimental flicker?
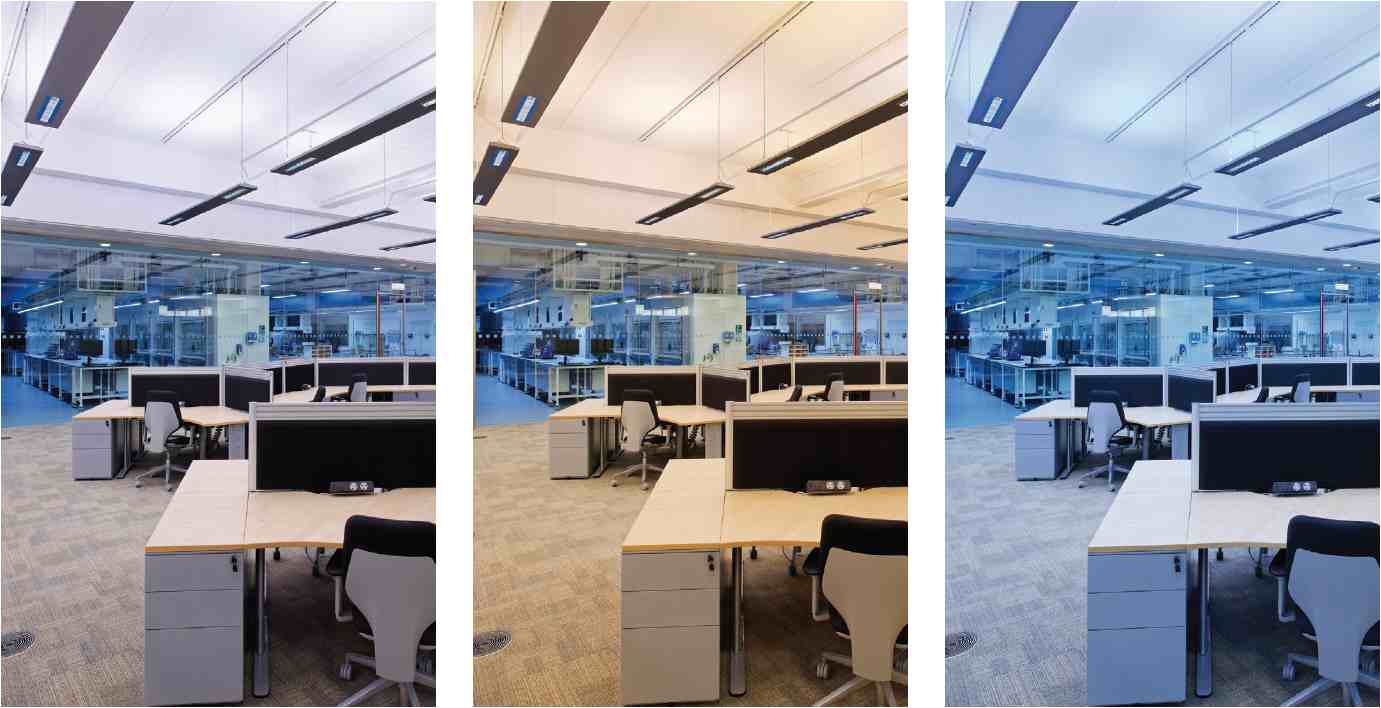
Dynamic lighting can be useful in spaces where there is a lack of daylight, to give people a connection with conditions outside. In 2010, Hoare Lea Lighting’s design for AstraZeneca used fluorescent lamps, with high-frequency control gear – so no flicker – to create different colour temperatures
So there are many unknowns and we need to be cautious. As a designer, I am concerned that these lighting systems are being installed now, when research is in its infancy. We should not forget that we already have a wonderful, rich, bright, wireless and free source of light that gives us all we need in terms of spectrum, infrared, UVA, UVB, illuminance, social interaction and psychological wellbeing: it’s called daylight. We can build intelligent lighting systems in our workplaces, schools, public buildings, care facilities – even our homes – but the fact remains that if you make sensible decisions about exposure to daylight, you will have a healthy circadian rhythm.
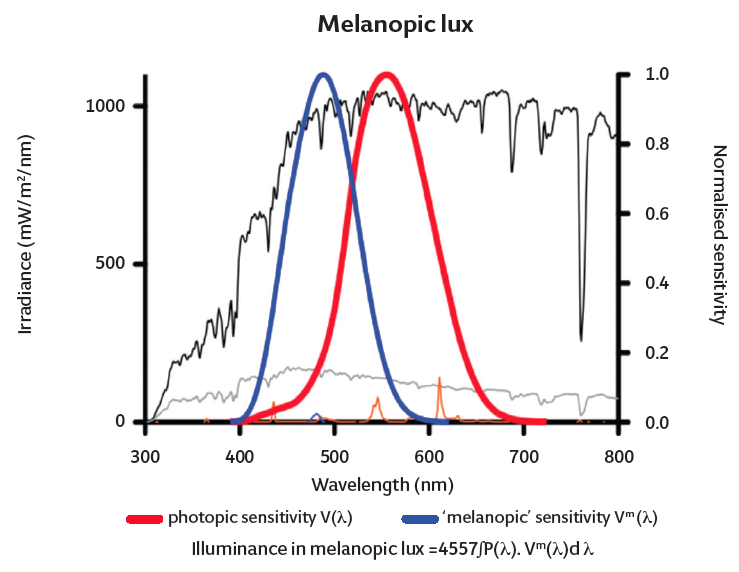
Courtesy of Robert Lucas, University of Manchester after al Enezi et al (2010)
So my advice is educate people about the need for daylight; make people move, get fresh air and understand the importance of ‘visual wind down’ in the evening, with warm spectrum, dimmed lighting easing sleep. Reduce the electronic devices used in your home in the evening and use blackout curtains to sleep in a dark environment.
We should also educate developers about daylight, and design spaces that people wish to use and illuminate them appropriately. Avoid the gimmickry of dynamic colour-mixing. Instead, consider designing a space that is ‘melanopic neutral’ – that does not have a detrimental impact on the circadian system – by avoiding warm spectrum light and dim illumination levels. Finally, wait for the scientists to test the impact of circadian light in care and dementia homes, and on shift workers – those with a real need. And, if the results are positive, then look at how to apply this knowledge to offices, homes and public spaces.
About the author
Jonathan Rush MSLL is a partner, lighting design, at Hoare Lea
References
- Al Enezi J, Revell V, Brown T, Wynne J, Schlangen L, and Lucas R (2011), Journal of Biological Rhythms, 26(4), 314-323.
- Lucas et al, Measuring and Using Light in the Melanopsin Age, 2014



