
People in the UK, as in most of the Global North, spend about 65% of their time at home, where pollutant concentrations can be much higher than in outdoor air.
A pollutant of particular concern is particulate matter less than 2.5µm in diameter (PM2.5). Exposure to this contributes to many serious health issues, including lung cancer, stroke, heart disease, and asthma.
PM2.5 is readily filtered with portable home air purifiers (HAPs) equipped with high efficiency particulate air (Hepa) filters. One potential way of improving air quality is by using smart building control systems to maintain a healthy indoor environment through automated windows and HAPs.
Researchers at the University College London Institute for Environmental Design and Engineering carried out a study that assessed the impact on health of using automated systems.
Health modelling was included to predict the potential scale of the impact of changes because of the framework
Occupants’ operation of windows exerts a substantial impact on indoor air quality and building energy consumption, but it also has the potential to conflict with air filtration strategies in buildings. Bearing this in mind, the study aimed to develop a novel building control framework that optimises the operation of windows and portable HAPs to improved energy efficiency and health.
Building control systems play a central role in building operations and performance. The overall goals of such systems are to satisfy occupants’ comfort and minimise building energy consumption and carbon emissions.
Building control systems, in general, share a common structure: sensor to controller to controlled device. The sensor measures an environmental parameter (for example, temperature and CO2 concentration) and sends collected data to the controller, which then processes the data with pre-programmed logic to determine the direction of change.
Window-control systems have become a hot research topic in recent years, as has the study of HAPs. However, an integrated system, which controls both window operations and HAPs, has not been explored.
Methods
The proposed control framework takes into account seasonality. For the non-heating period, the control framework has HAP and window controls running
in parallel.
In contrast, for the heating period, the window is set to be closed, while the mechanical ventilation with heat recovery (MVHR) system operates continuously to provide background ventilation, with the HAP control enabled.
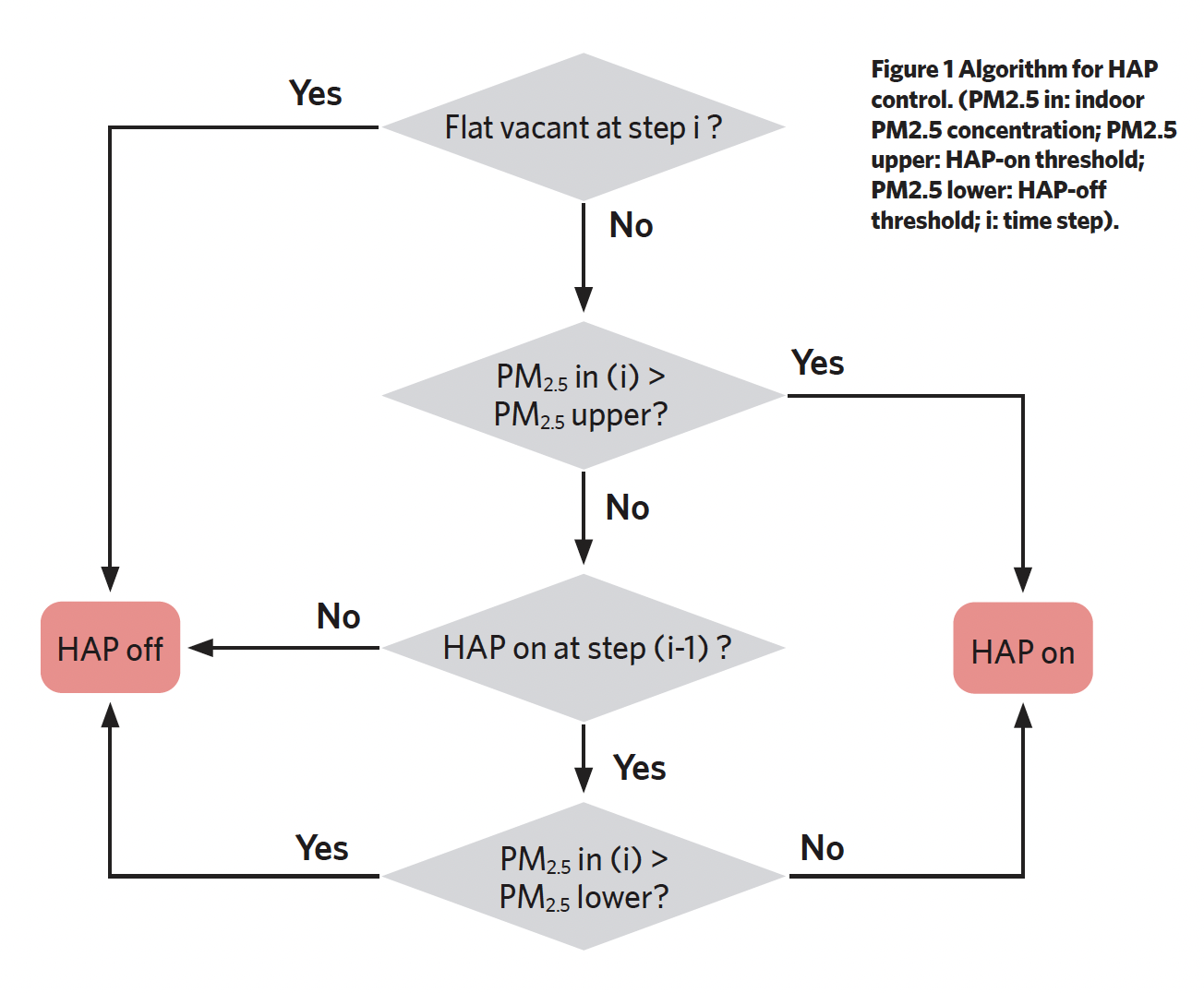
Schematic diagrams of the logic for HAP and window controls can be found in Figures 1 and 2. The HAP is set to run when the indoor PM2.5 concentration reaches the defined ‘HAP on’ threshold (15µg/m3) and stops working once the concentration falls below the defined ‘HAP off’ threshold (5µg/m3).
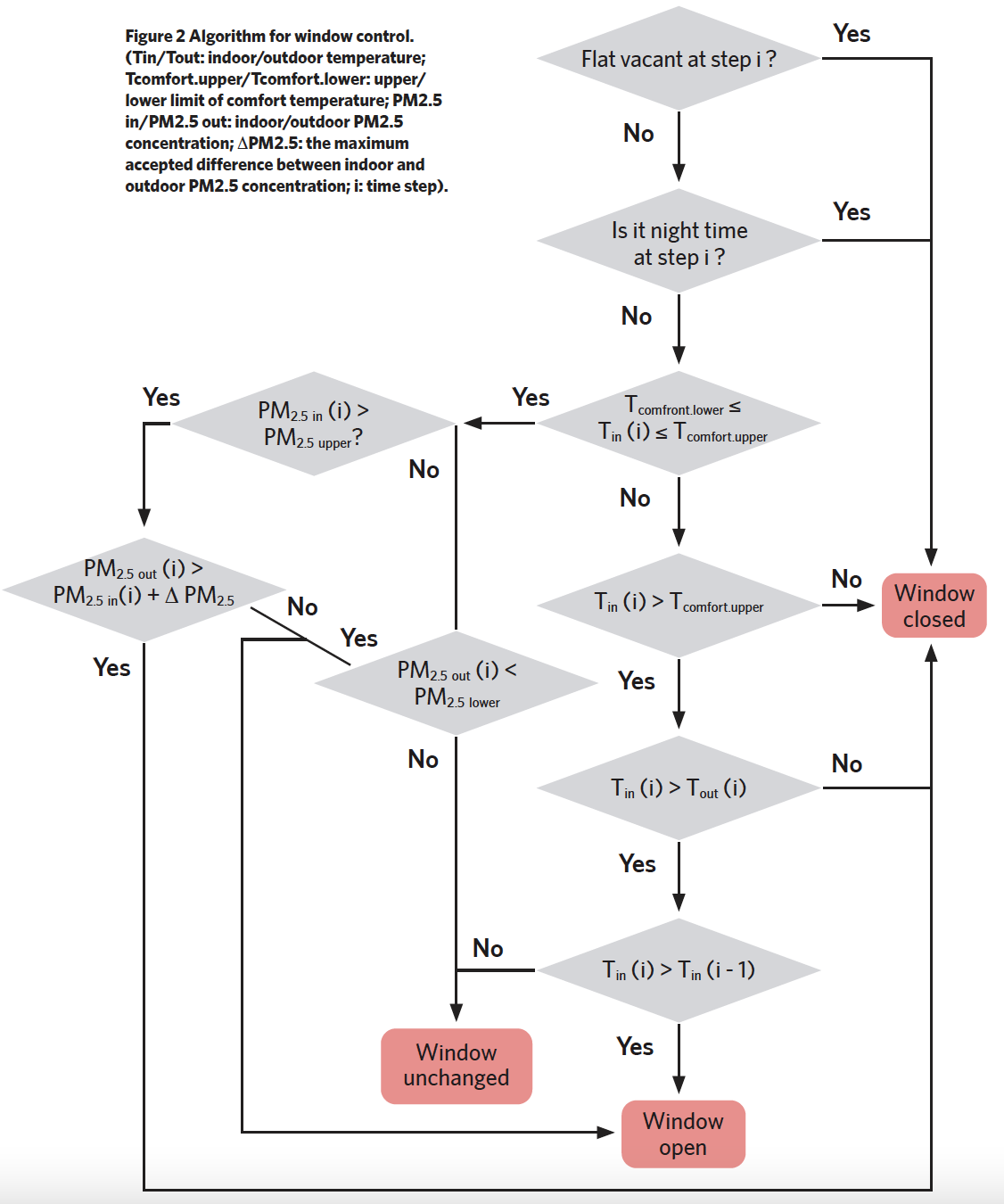
To maintain security, the window is set to be closed at midnight and when the residence is unoccupied; otherwise, the default state of the window is fully open to enable natural ventilation. The window is set to fully close when the indoor temperature falls outside the limits of EN 16798-1 Category II adaptive comfort temperature. Moreover, if the outdoor PM2.5 concentration is higher than that indoors, and the indoor temperature is within the comfort zone, the window will be fully closed to reduce the HAP working load.
Health modelling was included to predict the potential scale of the impact of changes because of the implementation of the control framework.
Quantitative health impact assessments are used to estimate future rates of mortality and morbidity from different interventions compared with what is predicted without such changes.
In the work presented here, life-table models were used to quantify the impacts on mortality of reductions in indoor PM2.5 concentrations.
The life-table method is based on age- and sex-specific mortality rates, which are used to calculate probabilities of survival by year of age and calendar year. An impact assessment is performed using the underlying mortality rates, which are adjusted to reflect changes in mortality risk from changes in exposure by applying relative risks calculated using available epidemiological evidence.
Individual single-year survival probabilities are multiplied together to calculate cumulative probabilities of survival over multiple years.
These cumulative survival probabilities are applied to a population, allowing the calculation of life years lived by the population (where one life year is a full year of life lived by one person), which, in turn, can be used to estimate the average remaining life expectancy per person by age.
Results
The proposed hybrid control framework – along with either HAP or auto-window control alone, for comparison – was tested in building simulations for a one-bedroom apartment. The simulation results for a summer week are presented below.
As seen in Figure 3, for the baseline scenario without any control measures, there were morning and evening peaks of indoor PM2.5 concentration; the daily mean of indoor PM2.5 concentration exceeded the World Health Organization (WHO) 24-hour limit (15µg/m3) for most of the week, while the indoor temperature stayed within the comfort range all the time.

For the auto-window control mode, the peaks of indoor PM2.5 concentration declined significantly with use of the auto-window control, reducing the number of days exceeding the WHO limit of PM2.5 concentration by two from the baseline. Meanwhile, occupant thermal comfort was satisfied. Yet, the results indicated that relying on window controls alone may be insufficient for cases of both high indoor and outdoor pollution levels.
In the HAP control mode, the peaks of indoor PM2.5 concentrations were significantly reduced. However, there were still two days when the daily mean concentration of indoor PM2.5 was above the WHO limit, even with the use of HAPs. The reason was that outdoor PM2.5 levels were considerably higher on those days and, therefore, leaving the window open worsened indoor conditions.
As shown in Figure 4, for the hybrid control mode – which represents the proposed control method – the indoor PM2.5 concentration decreased substantially, with no days exceeding the WHO daily limit, while indoor temperature remained within the comfort range.
The major advantage of the joint control of HAPs and windows was that the window could be shut when outdoor pollution was high without an accumulation of PM2.5. In this way, the HAP operation was minimised, and the indoor PM2.5 concentration was lowered. Meanwhile, the control algorithm was directed to look for opportunities, when the outdoor air was good, to open the window for natural ventilation.
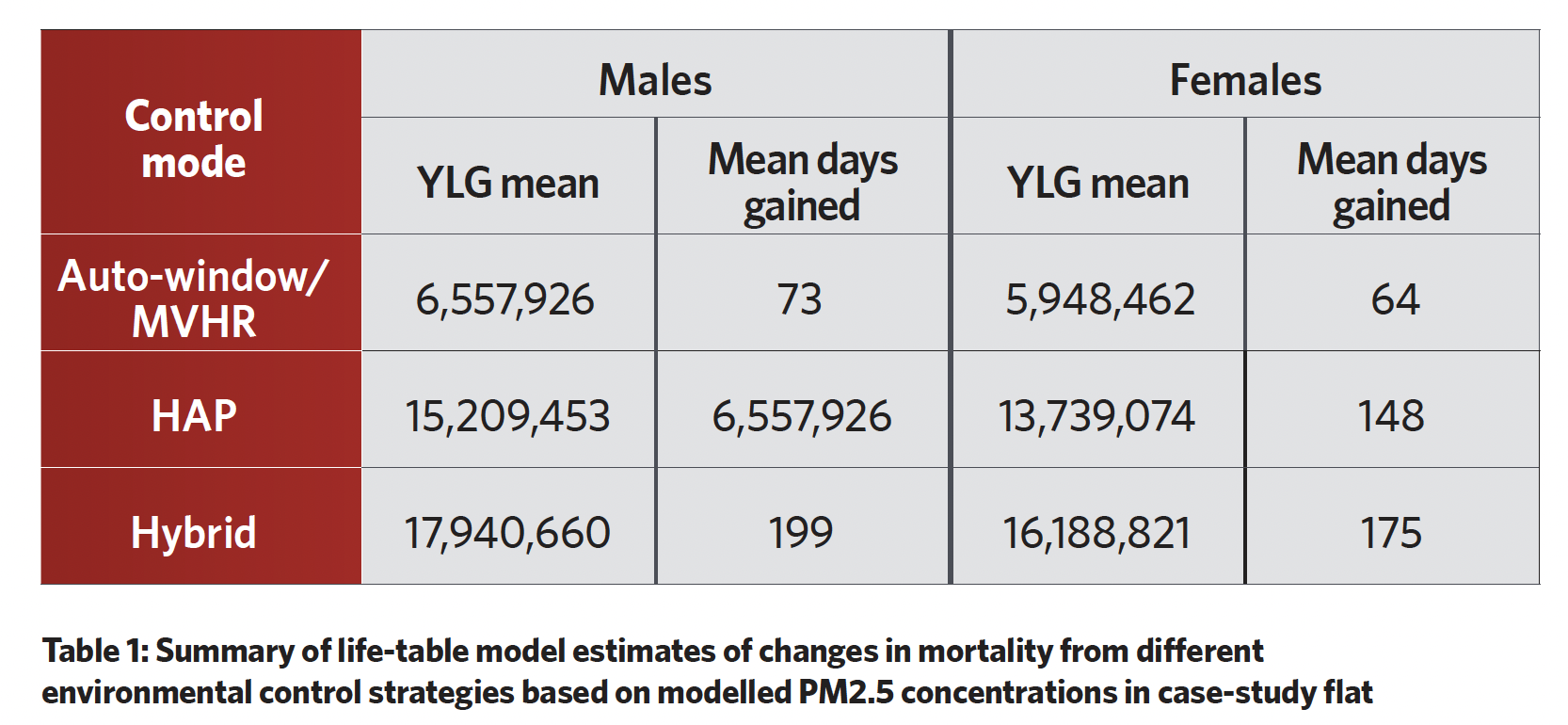
Based on the modelled indoor PM2.5 concentrations of the case-study flat, the mean years of life gained (YLG) for all males in the UK across the modelled period (97 years) were approximately 6.5 million, 15 million, and 18 million for the automatic window/MVHR, HAP, and hybrid modes respectively. The mean YLG for females over the same modelled period were approximately 6 million, 14 million, and 16 million for these three intervention scenarios, respectively (Table 1).
The reduction in exposure to PM2.5 from the implementation of the hybrid mode added a mean of nearly six months of life.
Key messages
The work presented here highlights the importance of building designers and engineers recognising health impacts, as well as energy efficiency and environmental impacts, related to occupant-centric building design and operation. The implementation of smart building control systems has the potential to reduce people’s exposure to PM2.5 indoors, which could have substantial health benefits.
This research adds technical evidence for policy-makers, to help prioritise health in the building sector. It also shows how smart and connected building control systems could improve indoor environments for better health of the occupants.
About the authors
Dr Elizabeth Cooper Lecturer MSc Health, Wellbeing & Sustainable Buildings, UCLs
Dr Yan Wang PhD student at UCL