
The NRC is on the Stanford Hall estate, home of the Defence and National Rehabilitation Centre
The NHS National Rehabilitation Centre (NRC) is a pioneering facility designed to provide intense rehabilitation programmes for up to 750 patients each year, to increase their chances of returning to life and work.
Currently being constructed at Stanford Hall near Loughborough by the Nottingham University Hospitals NHS Trust, the £105m building is the first hospital in the UK to target net zero under the NHS Net Zero Building Standard (NHS-NZBS). It is all-electric and features three R454 air source heat pumps (ASHPs) and 900m2 of solar panels, which are predicted to provide 10% of the building’s energy needs.
Project team
Client: Nottingham University Hospitals NHS Trust
MEP engineer, civil and structural engineer, and net zero carbon consultant: Arup
Architect: Ryder Architects
Main contractor: Integrated Health Projects (joint venture between Sir Robert McAlpine and Vinci Construction)
MEP contractor: T Clarke
The centre is pioneering a new interoperable building management system to demonstrate how smart technology could be incorporated into new and existing NHS hospitals and facilities. This is designed to talk to buildings’ engineering systems and, crucially, enable staff and patients to talk to it, literally, through voice-activated environmental controls.
‘We want to give the patients autonomy to be as comfortable as possible in their environment,’ says Ryan McCormack, head of programme construction and commercial for the NRC.
This pioneering new building was given the go ahead in September 2023. Its architectural design, however – including its irregular zig-zag, three-storey central spine, orientated along an east-west axis –had been conceived in 2016. The spine is home to the building’s double-height reception, while its ground floor contains the specialist treatment and clinic facilities, two gyms, a dining room and an innovation suite, which are housed in a series of pavilions projecting from the crooked core. The upper floors have a patient lounge and sleeping accommodation, arranged in individual rooms.

A visualisation of the dining room
There is a separate energy centre building, and landscaped gardens surround the facility to further enhance patient wellbeing. The Energy Centre only provides services to the NRC building and it is not connected to the DMRC. Majority of primary plant are included in the energy centre, such as air source heat pumps, generators, water tanks and medical gases. There also are some plant areas within the NRC that house air handling units.
The NRC was granted planning consent in 2018. In the period between this and the scheme being given the go-ahead, NHS England made a commitment to reduce the carbon footprint for its estate, targeting an 80% emissions reduction by 2028-32, and net zero emissions by 2040. The NHS-NZBS – published in February 2023 and referenced in the pilot version of the UK Net Zero Carbon Buildings Standard – is designed to meet that commitment.
It was decided that the NRC would retrospectively target net zero carbon under this standard. This was an additional challenge because the building’s irregular form – with its projecting pavilions of clinics and specialist treatment rooms designed to foster collaboration and innovative treatments – increased the surface area of the building envelope significantly.
‘The design team had to pay additional attention to insulation and airtightness to minimise any heat losses,’ says McCormack. ‘The SIP panels have been tested and shown to provide an air tightness of 1 in tested environment. This lead design team down the route of the final solution. The team also used analysis from energy model to optimise U-value to come up with optimum thickness panels,’ he explains.
Non-combustible, structurally insulated panels (SIPs) provide a high-performance, thermally efficient and airtight envelope, and help the scheme to comply with modern methods of construction targets in the government’s New Hospital Programme. The SIPs are clad in low embodied carbon fibre-cement panels.
In addition, the roof accommodates 900m2 of photovoltaic panels, estimated to produce around 185MWh of electricity per year.
The building’s low carbon design is further enhanced through the use of post-tensioned concrete to form the upper floor slabs. This has comparatively lower embodied carbon compared with conventional concrete floor slabs. A concrete raft slab forms the foundations and ground floor, and avoids the cost and high embodied carbon associated with a piled substructure. Although concrete is used throughout the building, its associated thermal mass was shown to have little effect on the overall building energy demand compared with other measures.

Natural materials are designed to make spaces feel less clinical and more comfortable
At RIBA Stages 2 and 4, building services engineers Arup undertook extensive design modelling to determine the impact of various passive design interventions. These included the use of high-performance glazing and solar shading on the south elevation to keep cooling loads to a minimum.
To target the NHS-NZBS, Arup developed an all-electric building services solution for the NRC, which factored in future changes to the climate over the lifetime of the building. As such, heating and cooling are provided by three R454 ASHPs, each capable of producing 439kW of cooling and 337kW of heating. For cooling, the energy efficiency ratio is 3.12 at 100% load and the low-temperature hot water coefficient of performance (COP) is 2.69 at 100% charge.
Backup generator
The NRC uses a large diesel-fed emergency backup generator. The use of batteries and other energy-storage devices were discounted because of the reliability of the technology and available space and infrastructure on site. It is hoped that when cost-effective, low carbon alternatives are commercially available, these would replace the diesel generator.
Dynamic simulation modelling was used to identify the times and conditions under which simultaneous loads occur, so that waste heat from the provision of cooling can be reused to provide heating, increasing system efficiency and enabling seasonal efficiencies in line with the net zero standard’s performance targets.
The lower-temperature heating circuit is kept separate from the higher-temperature domestic hot water (DHW) circuit to maximise system efficiencies. Six (CO2 refrigerant) ASHPs provide a total of 100kW of heat per heat pump at a COP of 2.25 @ -5°C and a COP of 3.1 @ 10°C.
To further improve efficiencies, the DHW system incorporates thermal stores to meet hot-water demand at peak times without having to oversize the heat pumps. These stores also help to reduce heat-pump cycling.
Mechanical ventilation with heat recovery is used for all spaces, with the exception of the isolation suites used for infectious patients. CO2 sensors located throughout the building deliver a demand-driven ventilation strategy, with systems ramping up and down accordingly as people move around the building. ‘If it’s hot within the building, or we have high levels of CO2, then we have the ability to measure that and control the ventilation,’ explains McCormack.
To give patients and clinicians additional control over their environment, and to reduce energy use, some areas of the building incorporate openable windows as part of a mixed-mode ventilation solution.
The centre is also designed to ensure high levels of daylight. To minimise energy consumption, the LED lighting system is linked to both occupancy and daylight-level sensors. ‘If it’s light outside, we don’t want the lights on in the building,’ McCormack says.

Patients are due to start moving into the building in summer 2025
Critically, patients are given control over the environment in their rooms through a digital tablet. As well as facilitating traditional entertainment streaming and phone calls, the tablet allows patients to control their window blinds, room lighting and temperature using voice control. ‘We’re looking at features to make controls as accessible for as many patients at NRC as possible,’ says Lisa Yates, digital strategy lead at Nottingham University Hospitals NHS Trust.
The tablet will also feed into the nurse call system to enable patients to request drinks and choose menus, or to be repositioned. Crucially for this facility, the tablet has the capability to guide patients through exercises, via games and other apps, to help speed up their rehabilitation.
The tablet is just one of 50 technologies that have been identified for new NHS buildings. Rather than install all of them at the NRC, however, the design team decided to focus on technologies that would be most beneficial in hastening recovery and improving the patient and staff experience.
To help identify these technologies, the hospital trust carried out trials at its current neuro-rehabilitation unit, the 25-bed Linden Lodge in Nottingham.
‘Until a technology has been implemented in a real, live, patient environment, we don’t fully know how it is going to work, and we need that feedback from patients and staff,’ says Yates.
‘The main point is to trial the proof of concept: do they deliver on the benefits we think they will, because we need to be confident in our procurement decisions for the NRC and, ultimately, for the trust.’
As a result of the trial, other digital technologies adopted include:
- A digital twin of the building to allow staff to identify, in real time, where a piece of equipment is within the building using an app with which they are familiar
- Digital signage so staff can see which rooms are available
- Artificial intelligence-enhanced CCTV that features ‘digital tripwires’ to help keep patients with cognitive impairment from absconding.
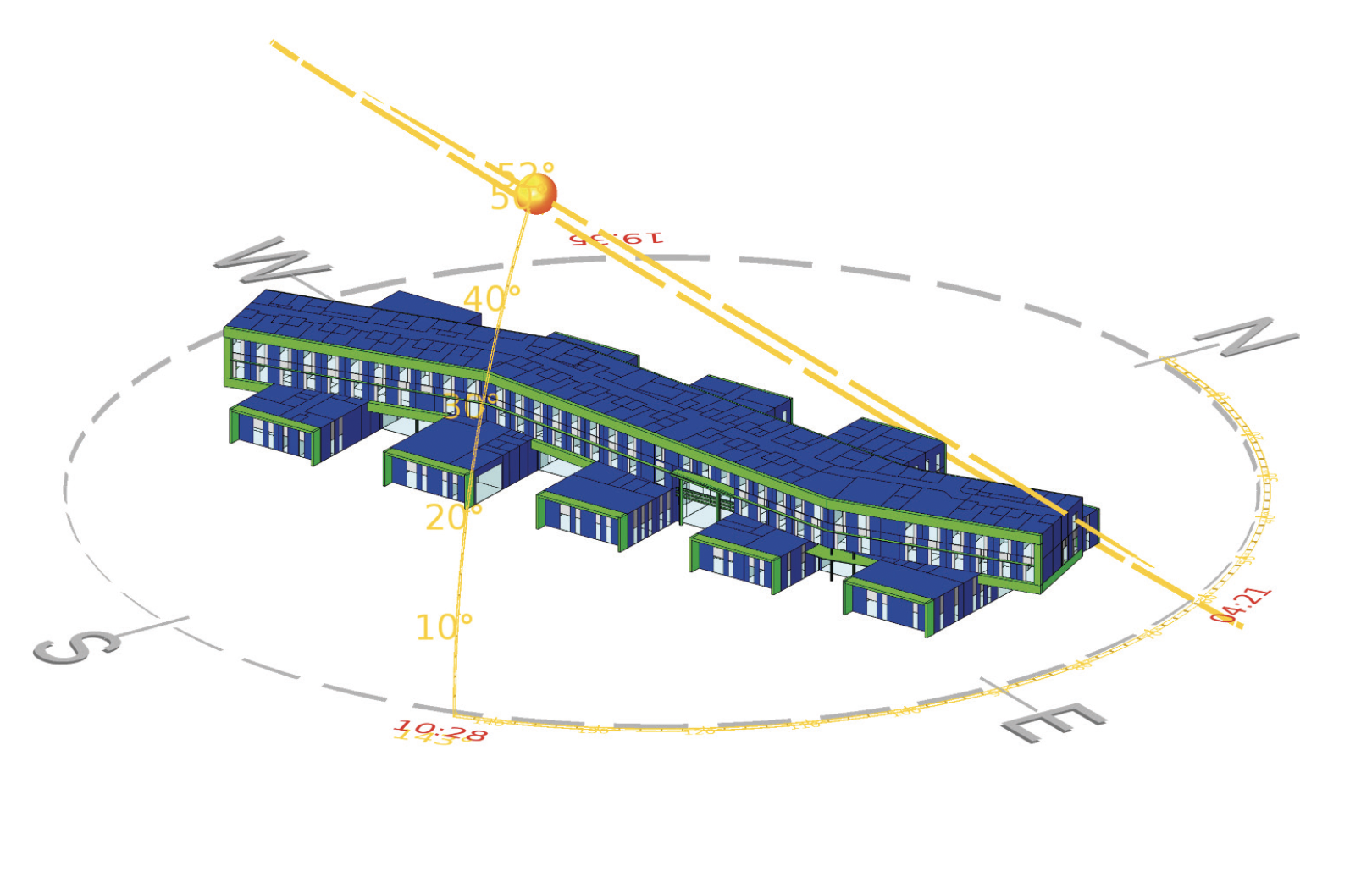
The building is orientated along the east-west axis
As well as gathering feedback on technologies that would be most appropriate for the NRC, the Linden Lodge trial also provided valuable insight into the challenges of installing the technologies in new and existing buildings – see panel, ‘General lessons learned from trialling technologies at Linden House’.
Lessons learned from trialling digital technologies at Linden House
- Smart hospitals require a large increase in connected devices, and many existing buildings don’t have enough power, data or containment to do this without considerable work.
- Aligning stakeholders to enable works to be completed at a convenient time, to minimise interruption to clinical operations, is challenging and causes delays.
- Different areas of the hospital have different infrastructure; lead-lined areas such as theatres and the emergency department mean additional network infrastructure is required.
- Changes to current processes need to be supported until new technology is truly embedded into daily practices.
- Staff engagement in the design process is essential. Digitally disenfranchised groups should not be further isolated by implementation of technology.
- Technologies such as nurse call and CCTV, security and access control cut across organisational structures, so it takes time to clarify which departments are responsible for which systems.
- Life-cycle costs need to be fully understood and mapped out, including battery changes for the Internet of Things and the true costs of cloud data.
- NHS governance processes are not agile, which restricts the ability to implement innovation at pace.
‘We’ve learned a lot about the constraints from being able to install these technologies in an existing estate – which will be the case for a lot of hospitals going forward, because they are not all going to go into brand-new shiny buildings,’ says Yates.
The NRC is set to receive its first patients later this year, at which point the design team will be able to establish whether the actual energy consumed by the building falls within the prescribed limits of the NHS-NZBS. Dynamic simulation modelling and whole life carbon analysis throughout the design phase strongly suggest it will.
NHS-NZBS targets for NRC