
The heatwave of 2003 – which peaked at 38.5°C in the UK – will be a normal summer by the 2040s, leading to related deaths more than tripling, according to the Committee on Climate Change (CCC) report published last month.
Currently no policies exist to ensure homes, schools and offices remain tolerable in high heat, and critical facilities – such as hospitals and care homes – are particularly at risk.
The paper Design and delivery of robust hospital environments in a changing climate – funded by the UK Engineering and Physical Sciences Research Council (EPSRC) – investigated the incidence of summer overheating in five hospital building types in the National Health Service’s (NHS’s) acute estate.1 Here, we focus on the 1983 Rosie maternity hospital, part of Addenbrooke’s in Cambridge, during the summers of 2010 and 2011, when it experienced elevated internal temperatures – increasingly an issue for the NHS.2

From analysis of its real and simulated performance – now and through the coming century – alternative corrective interventions were devised, with a focus on summer overheating. The full paper reports the relative costs and ‘value for money’ of four options.
The Rosie is a courtyard type of building: steel and concrete-framed, three storeys, with double-loaded racetrack corridors and brick-clad. Research identified 117 medium-rise courtyard examples in England, covering approximately 3 million m2.
In 2010, the – since refurbished – building was mechanically ventilated throughout the year, with a set point of 24°C. Air, which was maintained below 22°C all year, was supplied through corridors, and exhausted in wards, WCs and dirty utility rooms. Warm air heating was supplemented by perimeter hot water (HW) heating elements without local thermostatic control and with no zone control. The building provided chilled water to an air handling unit (AHU), but only delivered comfort cooling to intensive care units (ITUs) and operating theatres. Orientated east-west, the building’s main entrance, and many of the multi-bed wards – occupying the second and third levels – face south.
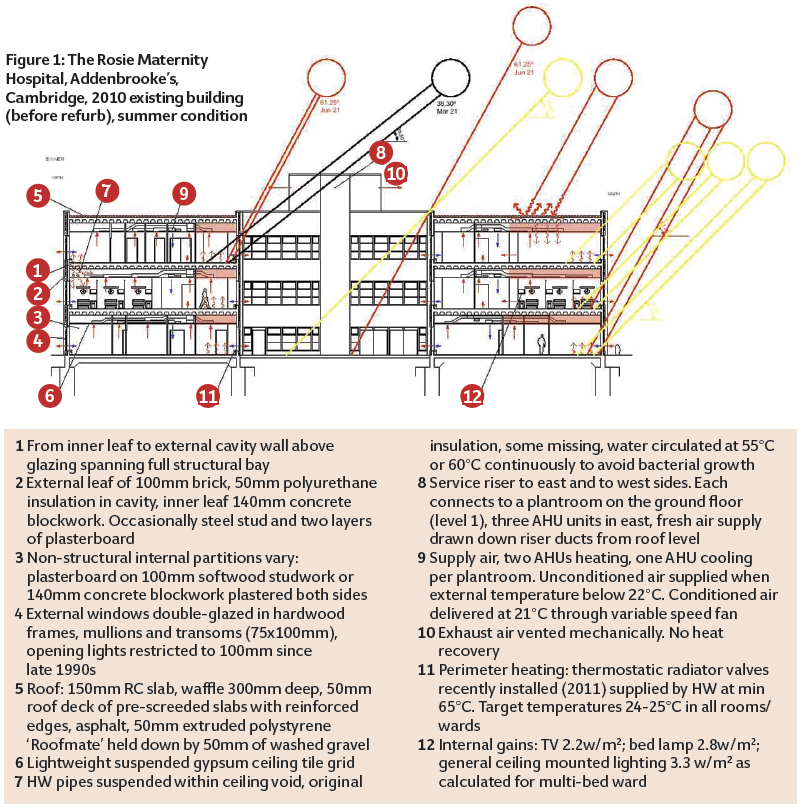
The researchers’ data loggers were placed on the second floor in June 2010. Figure 1 records factors that were observed to contribute to overheating, including: uninsulated steam pipes; internal heat gains from lighting and equipment; liberal glazing, largely fixed with a limited row of lights opening to only 100mm, exposed to direct solar radiation. Thermal comfort was marginal, even on mild days, in south- and south-westerly facing wards.
Carter Bronze Medal Award winner
This article is an edited version of the paper: A medium-rise 1970s maternity hospital in the east of England: Resilience and adaptation to climate change , which appeared in CIBSE’s technical journal BSERT. The paper won the 2016 Carter Bronze medal for most highly rated paper relating to application and development. The paper was written by Alan Short, Giridharan Renganathan and Kevin Lomas (University of Cambridge/University of Kent/University of Loughborough). CIBSE members can access BSERT free from the Knowledge Portal.
Project definitions of thermal comfort included the simple static guidelines and criteria described by CIBSE and the adaptive thermal comfort thresholds in BS EN15251. The appropriateness of these approaches and their relative credibility is discussed by Lomas and Giridharan, and considered in the recent redrafting of the health technical memorandum (HTM) 07-02.3,4
The existing building enjoyed relatively low energy and low carbon performance against the Department of Health (DH) guidance benchmarks – but at the cost of comfort, unable to shed heat in relatively mild external conditions.
Hobo U2 temperature loggers monitored 26 spaces on three levels at hourly intervals from July 2010 to October 2011. The second level emerges as the hottest floor, where logger AR2-SB202 recorded the hottest space at 30.7°C. Maximum ambient temperatures during the summers of 2010 and 2011 were 29.6°C and 31.2°C respectively.
The year 2010 was relatively cool. Night temperatures were consistently uncomfortable – 23.4°C to 26.1°C – and one bedroom recorded 1,992 hours above 25°C, 888 of which occurred at night. Simple threshold criteria miss this. In the 2030 Design Summer Year (DSY), the existing building has a mean night temperature in excess of 25°C. The mechanical ventilation rate is too low – in most bedrooms it does not reach a minimum value of 10 l/s/p.
To predict the annual frequency of overheating of the wards, and the energy demands and CO2 emissions in the current climate, the dynamic thermal model IES was used.5 The full paper records reasonable agreement between IES predictions and measured values.
Current and future weather files were created by the Prometheus research team at Exeter University, and the future probabilistic weather files were derived using UKCP09 data. A detailed account of this process has been presented elsewhere.6 Schemes intended to deliver greater resilience to hot summers were devised, starting with what appears to have become the enlightened – but questionable – industry standard Passivhaus-derived model.
Option 1: Sealed mechanical ventilation heating and cooling (SMVHC)
In this option glazing is sealed, airtightness improved, and 100mm of insulation added to the roof and external walls. Mechanical ventilation is operated to achieve the then DH recommendation of 6ach, with 60% heat recovery. DSY peak temperatures will oscillate around 28°C, so additional cooling capacity will be required and will become increasingly necessary. Does the building have the capacity to accommodate it? Predicted energy demand is high (Figure 5) and associated CO2 emissions very high – 130kgCO2/m2 (Figure 6). Almost two-thirds of this will result from its electrical demand, which will, of course, rise as cooling capacity is increased.
Option 2: Natural cross-ventilation retaining perimeter heating (NCVPH)
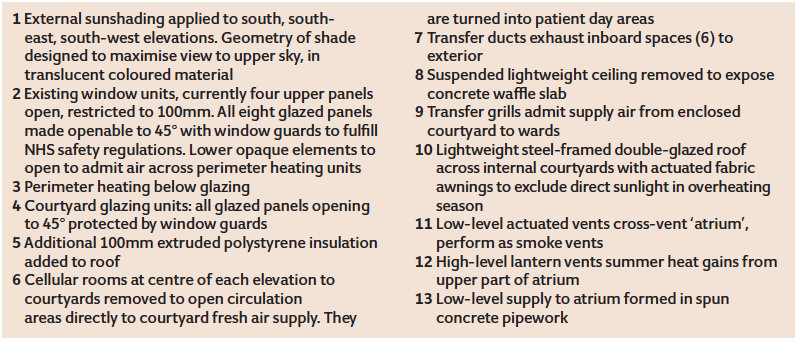
This reintroduces natural ventilation as the primary ventilation strategy (Figure 2): roof insulation is increased; all glazing to south – southwesterly and southeasterly elevations – is shaded externally, to a geometry that preserves bedhead-level views out; all glazed panels open to 45° (safeguarded with grillage); opening, opaque panels are added; and the whole recipe is repeated on the glazed courtyard elevations.
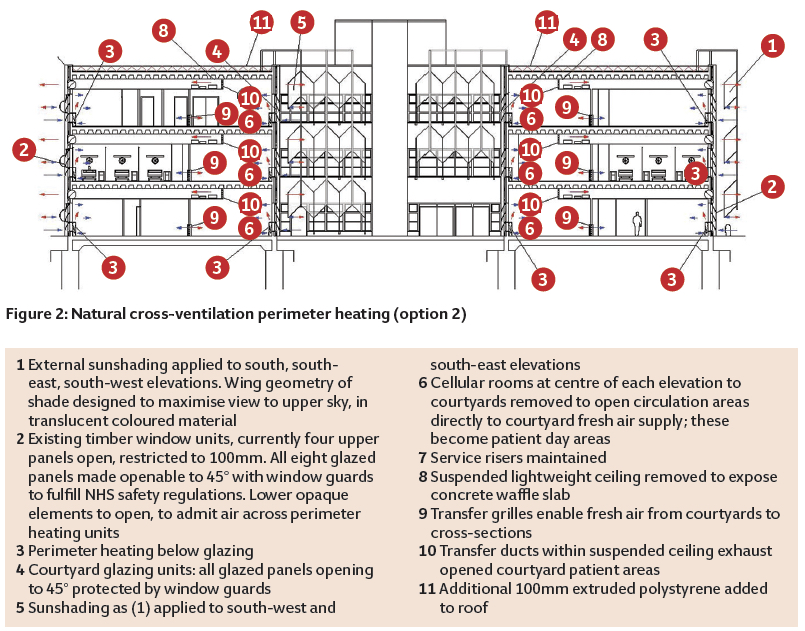
Spaces adjacent to the courtyards are opened, to enable distributed cross-ventilation by the removal of some cellular rooms to form larger, open, patient day-spaces. Suspended ceilings are removed in these areas to reveal concrete soffits that capture ‘coolth’ from cross-ventilation. Ducts connect these inboard spaces directly to the perimeter.
Peak DSY temperatures hover between 33.5°C and 34.9°C. Additional cooling will be required, but night ventilation cooling is wholly excluded by current set-point policy. A peak of 31°C is predicted in Test Reference Year (TRY) summer conditions. More research is required into clinically safe night conditions in maternity wards. Option 2 has the lowest energy penalty (Figure 5) and markedly lower CO2 emissions (Figure 6) than option 1.
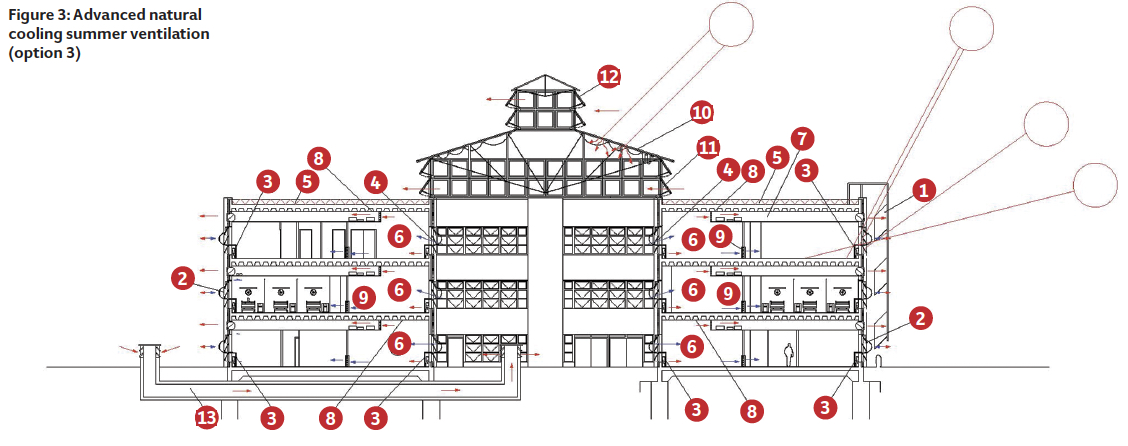
Option 3: Advanced natural cooling summer ventilation (ANCSVPH)
Courtyards are unheated, glazed atria with a liberal opening area above to dissipate summer solar gains (Figure 3). Air is supplied via concrete ducts below the ground slab, offering a measure of ground cooling. All glazing to the atria becomes operable to 45° and perimeter heating is retained. In winter mode, air is admitted through damper-controlled perimeter heating units. Transfer ducts exhaust air from zones adjacent to the atria and, as in option 2, suspended ceilings are cut back to expose thermal mass. All vulnerable glazing is shielded from direct summer solar gains. Option 3 offers similar DSY peak conditions as option 2, but TRY peaks within current guidance. Predicted energy demand and CO2 emissions are only marginally higher than option 2 (Figures 5 and 6).
Option 4: Natural ventilation incorporating Passive downdraught cooling and perimeter heating (NVPDCPH)
This option (Figure 4) also proposes enclosing the courtyards, but developing the low energy cooling strategy of the authors’ UCL School of Slavonic and East European Studies in London. Cooled water batteries at high-level openings induce a downward flow of pre-cooled air, contained by a lightweight, acoustically absorbent, fabric shroud. The cooled air is then drawn across surrounding occupied spaces.
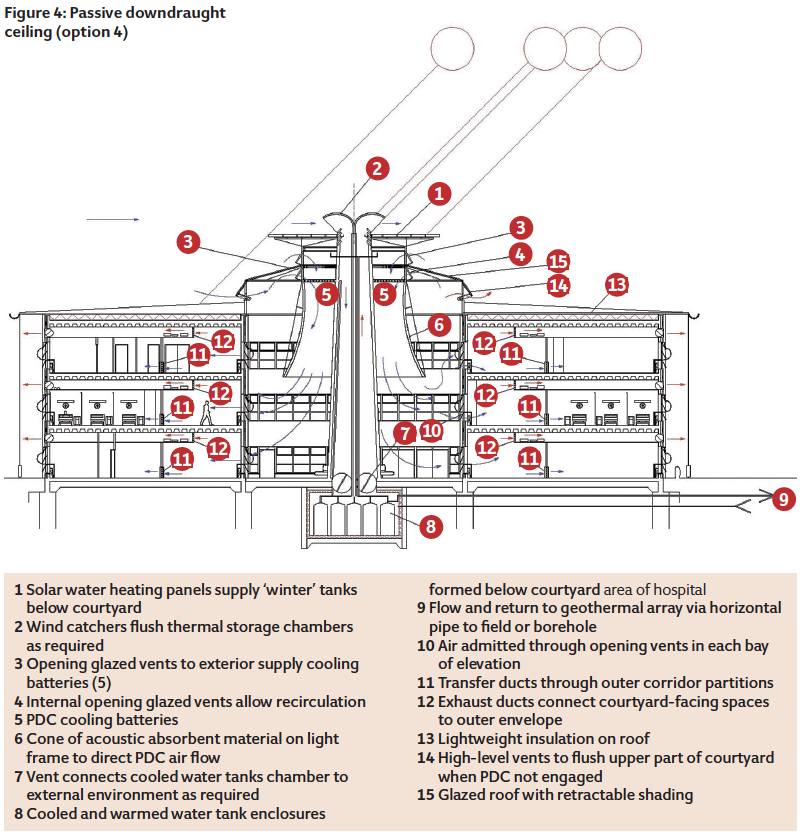
The diagram proposes ground-sourced cooling to supplement the action of the Passive downdraught ceiling (PDC) by using seasonal thermal storage, readily available water tanks, so that heat gained from summer hot spells is dissipated in winter, and winter coolth used in summer. Banks of passive solar water heaters on the roof of each PDC rooflight supplement warming of winter supply tanks. Recovered heat from all sources is gathered in winter to supplement the supply to the perimeter heating system. Option 4 offers lower TRY and DSY peaks than options 2 and 3. Energy input is higher, but the CO2 penalty is in line with options 2 and 3 (Figures 5 and 6). This is a complex option to model.
During extreme years, DSYs, option 1 (not illustrated) projected the best performance, while the 2010 building exhibited the worst performance. For the current DSY extreme conditions, all four options broadly met the HTM 03 1%/28°C, while – for the 2030s – option 2, 3 and 4 exceeded the criteria. But improved performance is achieved at a cost. Although the 2010 building, unaltered, had the worst thermal performance, it had the lowest energy consumption (Figure 5).
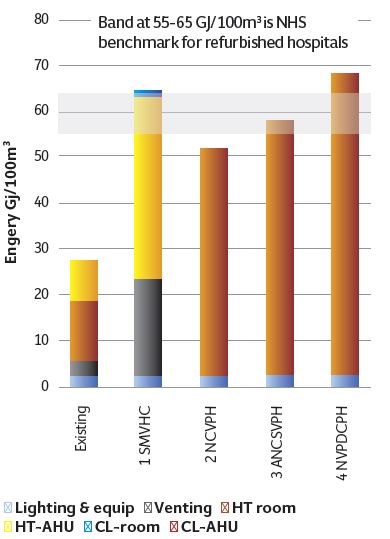
Figure 5: Predicted energy demand for existing and refurbishment options for the year 2010, Cambridge (Bedford weather file). The energy values are the average of monitored and modelled spaces AR1-EX, AR2-MB2 and AR3-DR
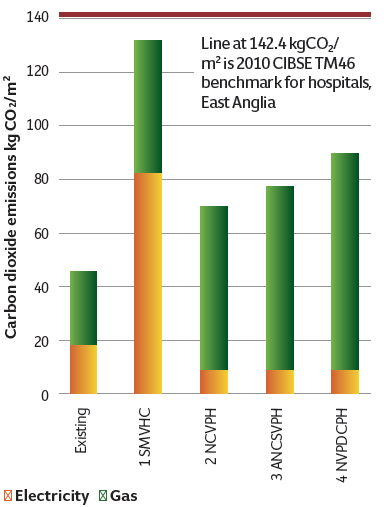
Figure 6: Predicted CO2 emissions for existing and refurbishment options for year 2010, Cambridge (Bedford weather file). The CO2 values are the average of monitored and modelled spaces AR1-EX, AR2-MB2, and AR3-DR
The DH Energy Efficiency Fund Scheme of 2013-14, which Alan Short administered in part, would not have funded any of the options; the Treasury requires a return on investment of 2.4 within five years of implementation. This is potentially a major barrier to achieving the adaptation of the public, non-domestic building stock – which is unfortunate given that the NHS Retained Estate seems a particularly promising place to implement a public sector adaptation scheme.
Acknowledgements
The authors would like to acknowledge the contributions of Phil Nedin and Shahila Sheikh, mechanical engineers at Arup; Paul Banks and David Nichol, quantity surveyors at Davis Langdon Aecom building cost consultants; Short and Associates Architects for producing adaptive design drawings; colleagues engaged in the EPSRC project; the Addenbrooke’s hospital estates and facilities department; and the staff of the Rosie for their forbearance during data collection.
- This article was written by Alan Short, University of Cambridge; Renganathan Giridharan, University of Kent; and Kevin Lomas, University of Loughborough
References:
- Short CA, Lomas KJ, Giridharan R and Fair AJ Building resilience to overheating into 1960s UK hospital buildings within the constraint of the national carbon reduction target: adaptive strategies, Building and Environment, 55, pp73-95 (2012) 10.1016/j.buildenv.2011.12.006
- Heatwave Plan for England 2014. Protecting health and reducing harm from severe heat and heatwaves. Public Health England, May 2014, downloaded 23 October 2014.
- Lomas KJ ,Giridharan R, Thermal comfort standards, measured internal temperatures and thermal resilience to climate change of free-running buildings: a case study of hospital wards, Building and Environment, 55, pp57-72 (2012) 10.1016/j.buildenv.2011.12.006
- The guidance on energy efficiency for the NHS, Health Technical Memorandum (HTM) 07-02, published in March 2015.
- Integrated Environmental Solutions (IES) (2010) IES VE Software Version 6.4, accessed 23 February 2012.
- M Eames, T Kershaw, D Coley (2011), On creation of future probabilistic design weather years from UKCP09, Building Services Engineering Research and Technology 32 (2) (2011) 127-142.
- NHS Energy Efficiency Fund 2013-14, adjudicating the distribution of the £50m fund across NHS England, with the professor of sustainable engineering, reporting to the under-secretary of state for health. The executive summary was published in February 2015.
