
The past decade has seen significant advances in our understanding of how environmental factors affect our health and wellbeing, and in design solutions in the built environment.
Combined with worldwide trends such as increased life expectancies, ageing populations, pressures on healthcare systems and the growth in urban living, these developments have prompted a significant revision of CIBSE guidance on health and wellbeing considerations in building services – Technical Memorandum 40 (TM40) Health and Wellbeing.
TM40 is now in the final stages of production, and this article summarises one aspect: the approach for defining indoor environment criteria for health and comfort. The TM will also include guidance on design, construction and operation. For an overview of the revision, see CIBSE Journal March 2018. Regular updates are provided at the CIBSE Knowledge Portal.
Defining performance
A significant update in the TM is the focus on building performance outcomes – for each environmental factor (light, humidity, thermal condition, and so on), the TM summarises existing health-based guidance and regulations, and proposes recommended levels accordingly. These levels may be used as targets, for example in new buildings, fit-outs and refurbishments, or as benchmarks in existing buildings to define priorities and short-to-longer-term improvement programmes.
In some areas such as air quality, this is a significant shift from the current approach – the term ‘air quality’ is often used when actually referring to design measures (ventilation rates); indicators (for example, total volatile organic compounds (tVOCs)); or occupant perceptions (for example smells, and complaints of ‘stuffiness’), as illustrated in Figure 1.
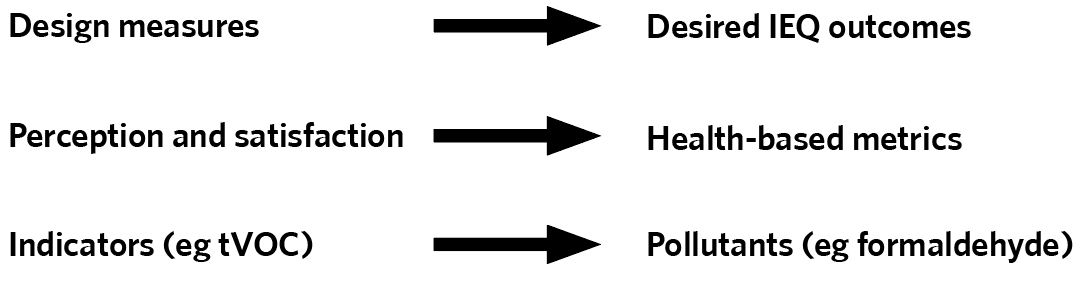
Figure 1: TM40 approach to performance criteria
Ventilation and indicators without consideration of potential indoor and outdoor pollutant sources are no guarantee of good indoor air quality. Similarly, while occupant feedback is useful to gauge comfort and satisfaction, it does not guarantee health-based outcomes. A stark example is carbon monoxide, which can be lethal but is not detected by human senses.
This TM intends to set out clearly health-based metrics to better inform projects and encourage a more rigorous common language. It also recommends avoiding the term ‘sick building syndrome’, which covers a range of possible symptoms and causes, rather than being specific about what the problem (and therefore the solution) may be.
For health purposes, as a very minimum it recommends meeting regulatory requirements and internationally recognised health-based guidelines from the World Health Organization (WHO) or its recognised agencies, as in the case of electromagnetic fields. This is broadly consistent with other emerging guidance, such as BS ISO 17772, 2018, and the revised BB 101: Ventilation, thermal comfort and indoor air quality 2018.
In many cases in the UK and EU, regulations incorporate – and are more onerous than – WHO guidelines; however, a notable exception is indoor air quality, where there are currently no comprehensive regulations, so professionals are therefore strongly advised to refer to WHO guidelines.
For comfort purposes, the recommendations in the new TM largely follow existing best-practice guidance. They stress the importance of user choice and control over their environment, to take account of individual sensitivities and preferences, increasing the likelihood of high comfort and satisfaction levels. This is not a new recommendation, and a large body of evidence from decades of post-occupancy evaluation supports it.
Looking ahead
There is still much debate, research and development in a number of areas, where professionals should be aware of the current limits of knowledge and where they can also seek opportunities for innovation, collaboration with academia, and added value to their clients.
One very active area is research on the impact of indoor environmental factors on cognitive performance, particularly in commercial offices. Studies vary greatly in quality – often, those that appear to offer new findings merely reiterate existing guidance, because the improvements in performance are shown by comparison with poor quality environments. Figure 2 illustrates recommendations from the TM on how to approach these studies.
Two of the main debates concern what should be the right limits for internal CO2 levels, and how to define and design for ‘human-centric’ lighting.
Traditionally, internal CO2 level has been seen as indicator of ventilation effectiveness rather than a pollutant in itself, except at very high levels. There is no WHO guideline limit on it, and UK regulations have occupational exposure limits (COSHHH – WEL) to prevent high CO2 levels leading to headaches, dizziness, confusion and loss of consciousness (5,000ppm for an eight-hour exposure and 15,000ppm for a 15-min exposure).
Many studies on the impact of indoor air on cognitive performance focus on ventilation rates, which makes it difficult to attribute changes in cognitive performance to CO2 levels on their own, as a range of other factors may vary with ventilation.
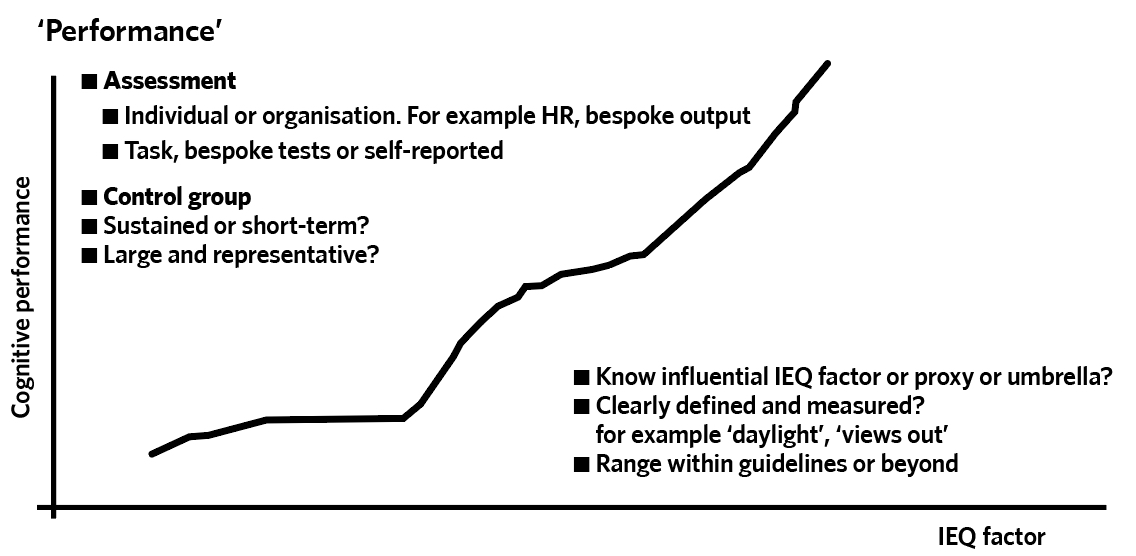
Figure 2: Studies on indoor environmental factors v cognitive performance: tips on what to look out for
However, recently a small number of studies have ensured that CO2 levels were the only variable by keeping ventilation rates and all other parameters the same, and simply introducing higher CO2 levels into the supply air. Most (but not all) tests show an impact on cognitive performance at increased CO2 levels, in particular on decision making, indicating that CO2 has an impact in its own right, and at lower levels than may have been assumed in the past.
However, it is also important to note that the levels at which significant effects are reported are well above existing best-practice guidelines (which are in the range of 750 to 900ppm).
Another very active area of research is ‘circadian’, or ‘human-centric’ lighting, where advances in our understanding of the non-visual effects of light on our health and alertness have prompted much debate about what the right metrics and levels should be. There is a general consensus that traditional measures of light, such as illuminance, are inadequate to represent the non-visual impact of light, and new metrics are therefore needed.
However, what these new metrics should be is still debated because of the complexities of our responses, interactions between different light receptors in our eyes, and time factors, which mean that a single light condition is not linked to a single response. There is no wide consensus yet; in the meantime, good design principles should be followed by seeking to give priority to daylight and views out (with glare control). It should be completed by electric lighting, which again should follow guidance from the SLL, including on parameters such as spectrum distribution, colour rendering and products.
Finally, an important conclusion from the evolving knowledge is that, in current projects, we should follow the precautionary principle to avoid unintended consequences, as those mainly only manifest themselves in the long-term – as in the case of asbestos and lead paint. This does not prevent innovation, but encourages a cautious review of claims, and possible effects, with monitoring and evaluation to keep new uses under review.